
EDITION: Bad New Times.
The disproportionate destruction of racialised communities through Covid-19 is the continuation of the colonial violence of which Florence Nightingale was a part.
Nightingale and neglect
On the 3rd April 2020, as the novel coronavirus pushed Britain deeper into crisis, government officials opened a new field hospital in east London. The ceremony made for surreal viewing; a handful of notables scattered awkwardly across an empty car park, dwarfed by the vast, hastily-converted conference centre behind them. Amongst those offering short speeches to the press was the Chief Nursing Officer, Ruth Mays. Despite reports in the morning newspapers that Britain had just experienced its ‘deadliest day so far,’ Mays’s speech was curiously unconcerned with the present. Instead, the majority of her comments focussed on the past, and the history of the new hospital’s namesake;
Next month will see the birth of Florence Nightingale - 200 hundred years ago - and its very fitting that this hospital is named [the] Nightingale Hospital London. She was well-known for being an iconic nursing leader and caring for soldiers in the Crimean war. What she was also, of course, [was] a pioneer for infection control and here having her name heading up this London hospital is absolutely fitting.
It is interesting that, amidst the worst public health crisis in living memory, Mays devoted her speech to remembering someone who was long since dead. Despite countless examples of selfless care, commitment and ingenuity amongst her own contemporaries, Mays chose instead to look to Nightingale for inspiration. Mays was not alone in making such a gesture. Prince Charles, addressing the ceremony by video-link, also spoke about Nightingale, claiming that, like ‘The Lady with the Lamp,’ the hospital would serve as ‘a shining light’ in ‘this dark time.’
It is strange to see Nightingale remembered like this, as a patriotic blur of field hospitals, wounded soldiers and gentle lamplight. This heroic montage obscures the comparative brevity of its source material – Nightingale, after all, spent just twenty-one months in the Crimea. While this brief period dominates all memory of Nightingale, no one so much as mentions the subject which occupied her thinking for the next forty years of her life; the British Raj, and India.
To remember Nightingale as a selfless nurse is to forget her as an avid colonialist, as an idealist who saw public health as the heart of the civilising mission. The image of the great humanitarian covers the racist reality; that Nightingale considered disease to be a product of filth and ignorance, and saw Indians as racially predisposed to both. Such opinions did not make Nightingale exceptional – indeed part of the reason that she should be remembered is that her opinions reflected the orthodoxy of the time. British public health in the 19th century was defined by racial logics, all tested and refined in the great social laboratory of the colonies. Theories of health and disease, purity and filth, risk and immunity, were all worked out in practice by colonial researchers, physicians and administrators. What makes Nightingale important is that she encapsulates the ideas of a moment – her thinking represents the ideological mainstream of British scientists and colonial administrators in the second half of the 19th century. Nightingale should thus not be remembered as an utterly exceptional nurse, but rather as an entirely typical colonialist.
The act of forgetting is really a failure to remember. Failure, in a colonial setting, usually means the negligence of the coloniser manifesting itself as violence against the colonised. Reflecting on the famine of 1865 to 1866, Lord Salisbury, the Secretary of State for India wrote that, “I did nothing for two months . . . it is said—a million people died. The Governments of India and Bengal had taken in effect no precautions whatever.”1 The violent negligence of the British was a consequence of their certainty in the less-than-human status of those they rule over. The lives of racialised Indians were not only worth less than the lives of their white British counterparts, but also worth less than their time and money. When the Lieutenant Governor of Bengal, Sir Richard Temple, bought rice from Burma to prevent a famine in 1873, the colonial establishment was outraged at this absurd “extravagance.”2 Senior civil servants denounced Temple, claiming it was a “mistake to spend so much money to save a lot of black fellows.”3
As a system, the British Raj always ultimately valued the exploitation of Indian labour above the continuation of the Indian lives that provided it. For the British, the lives of Indians were simply not valued as those of full human beings. To quote Achille Mbembe, “The savages are, as it were, ‘natural’ human beings who lack the specially human character, the specially human reality, so that when European men massacred them they somehow were not aware that they had committed murder.”
To fail to remember this history is to contribute to the violent neglect of the lives of the racialised and the colonised, then and now. It is also to neglect the foundations of those actions that are taken, the colonial origins of the coercive and carceral operations that complement and augment the violence of inaction. The disproportionate destruction of racialised communities through Covid-19 is the continuation of this violence in the present, and it is dependent on the violent neglect of the past. The fact that the “death rate among British black Africans and British Pakistanis… is more than 2.5 times that of the white population” is the latest manifestation of a exploitative neglect that depends on the continual destruction of its origins. Britain is forever losing parts of its colonial archive. This is a strategy to guarantee neglect, to prevent a critique of the past informing a critique of the present. The failure to remember is an act of political warfare, not least when it is the descendants of the colonialists that are overseeing the deaths of those descended from the colonised.
‘The handmaid of civilisation’
Nightingale’s entanglement with India began almost as soon as she returned from the Crimea. On the 10th May, 1857, Indian soldiers in Meerut mutinied, killing a British colonel and his family. Mutineers on horseback carried the rebellion down into Delhi, and out into the villages. By the end of the month, the East India Company had lost control of a “vast swathe of territory between Patna in the East and Patiala in the West.”4 Like much of the British establishment, Nightingale was quick to grasp the possible implications of the Mutiny. In July 1857, Nightingale wrote that;
As the revolution of 1793 in France was but the beginning of what ended in the total overthrow of the feudal system, so this affair in India must end in the entire doing away of the caste system or in the overthrow of the British power there. We may have to reconquer India. I should like much to go out.5
For Nightingale, and for the British in general, the Indian Mutiny presented an existential threat to the persistence of colonial rule. Nightingale’s prediction was prescient; the old system could not continue, and a re-conquest would prove necessary. In 1858, after a reconquista defined by its spectacular brutality, the old regime was replaced with a new one. The private rule of the East India Company was dismantled, and the state assembled the British Raj in its place. Nightingale represented the dominant ideology of the new order, and was deeply enmeshed in its system of power. Not only was Nightingale a close advisor of two Viceroys of India - John Lawrence, (1864-1869), and Lord Ripon (1880-1884) she was also a personal friend of both Sir Charles Trevelyan, governor of Madras, and Sir Bartle Frere, the governor of Bombay.6 As an icon of both liberal concern and scientific reason, Nightingale encapsulated the desires of the new order, for a more rigorous, more rational, approach to the project of ruling, and civilising, India.
Crucial to this new British Raj was a historic shift in the colonial approach to public health. The historian David Arnold has argued that the 1860s saw the beginning of a seismic transition from British medicine’s ‘enclavist origins’ towards a “pervasive system of . . . public health.”7 This general shift is noticeable in Nightingale’s writings. While Nightingale had initially only been concerned for the health of British troops in the severe conditions of the “tropical dominions,”8 she rapidly came to realise that the army could not expect good health if its surroundings were unhealthy.9 As Gérard Vallée has written, Nightingale’s ‘attention to the sanitary state of the ‘‘native lines’’ or ‘‘native lanes’’ then led step by step to a concern with the entire civilian population.’10 As early as 1857, Nightingale had realised the potential of health as a means to consolidate British power, a civilising tool that could guarantee the continuation of the colonial system:
The observance of sanitary laws should be as much part of the future régime of India as the holding of military positions or as civil government itself. It would be a noble beginning of the new order of things to use hygiene as the handmaid of civilization.11
1858 marked a turning point in how the British conceptualised colonial health. From this moment onwards, the British began to consider the health of the colonised as a crucial instrument in the reproduction of the Raj. As Nightingale was to write later, the British were “conquering Indian anew by civilisation, taking possession of the Empire for the first time by knowledge instead of by the sword.”12
This new interest in colonial health was matched by a reinvigorated study of the native population, which was characterised by its reliance on racial logics. Arnold has argued that, as an enclavist obsession with European vulnerability gave way to a more general, all-encompassing enthusiasm for public health, the causes of vulnerability themselves were rewritten. As basic reforms improved the health of British troops and officials, colonial opinion shifted away from viewing the environment as the cause of disease, and towards seeing poor health as a consequence of the “moral and cultural problems” of the native population.13 The Royal Commission report, to which Nightingale was an important contributor, noted that “the habits of the natives are such that, unless they are closely watched, they cover the whole neighbouring surface with filth.”14 Nightingale herself writes scathingly about the “filthy customs”15 and “foul native houses and inhabitants’ of India”,16 which she blames for plague and pestilence being “the ordinary state of things” on the subcontinent.17
This shift was partly powered by the increasing dominance of ideas of natural selection and evolved racial difference, as produced and popularised by Georges Cuvier and Charles Darwin. By the 1880s, William Aitken, arguably the most influential doctor in the Empire, was writing that the ‘gradual evolution’ of disease was inseparable from ‘the development of civilisation. As Michael Antolin has argued, medicine used Darwin’s theory to establish ‘“constitutions” and “diatheses” that characterized patients as being susceptible to particular kinds of diseases.’ These “constitutions” were understood to be a result of either “past natural selection or through degeneration back to atavistic traits.” Unsurprisingly, ‘this kind of typological thinking’ led to what Antolin acknowledges was explicit “racial profiling.” By the 1890s, public health in India had arrived at an understanding of disease as a product of the innate racial characteristics of the Indian population.
In the 19th Century, the British experienced two moments in India in which the very continuation of colonial rule was threatened. Both of these moments led to profound transitions in British approaches to the health of colonised and racialised peoples. If the first of these came with the Mutiny in 1857, the second arrived almost exactly 40 years later.
Coercion against contagion
On Saturday the 18th September 1896, an Indian doctor, Acacio Gabriel Viegas, attended a house call in the centre of Bombay (now Mumbai).18 His patient had a series of alarming symptoms; fever, impaired speech and an enlarged node in her groin. Later that day, Viegas was called to another patient, this time in the port district of Mandvi. The young boy he examined had the same list of symptoms. On Sunday, Viegas found his first patient dead, and the second much sicker. From the young boy’s uncle, Viegas learned that 50 people had died of similar symptoms in the last month alone. The other strange thing, said the man, was that all the rats seemed to be dying too. Viegas rushed to a laboratory and, through a microscope, saw tell-tale pink bipolar bacilli. The doctor immediately contacted the authorities, and told them he had found the bubonic plague in Bombay. Viegas’s speed and concern, was, unfortunately, not matched by the British. It took five days for a committee to even read the doctor’s report. When the British eventually reviewed Viegas’s submission, the information it contained would not have been a surprise to them – it appears that the authorities had been quietly shelving reports of plague from local doctors since May.18
The way the British responded to the plague in Bombay was defined by four aspects. Each of these have, in some way, been replicated in Britain’s current response to COVID-19. The first impulse of the colonial authorities was to deny and delay. After months of suspected cases, the British only eventually acknowledged the presence of the plague on October 1st. Even then, as Arnold notes, the official announcement stressed the disease was of a “mild” type.19 It took until October 12th for the British to get laboratory confirmation of the plague – a consequence, in part, of the fact that Britain had only one full time bacteriologist in the whole of India, Waldemar Haffkine, who had to travel from Calcutta to Bombay.
Such inaction undoubtedly worsened the course of the pandemic. By late Autumn, British officials were recording a thousand plague deaths a month, by early 1897, it was five hundred a week. Between October 1896 and February 1897, 380,000 people fled the city.20 Horrified officials watched as the city’s booming industry came to a choking halt; by 1897 only a fifth of Bombay’s millhands remained at work.21 Horrified by this extraordinary exodus, British officials began to discuss the possibility of the “absolute ruin of the city.”
The horror of the British officials, however, was not dictated by a moral concern for the destruction of human life. Instead, their initial inaction and subsequent horror has to be read in the context of the two centuries of famine and disease that preceded it. In India, violent neglect was defined by a constant calculation, one that observed the mounting death toll, but considered it in terms of its effect on the columns of colonial accounts. Action from the authorities only occurred at the point where the economic cost of doing nothing outweighed the cost of doing something.
In Bombay, the lives of the Indian population clearly mattered less than the labour they provided, and the denials and delays of the British stemmed from a fear of the effect of plague on the city’s industry and trade. This defined the second aspect of the colonial response – a constant prioritising of the economy over the lives of racialised, colonised people. The British were committed to preserving the function of the city’s textile mills and its vast port, and were willing to accept deaths as an unavoidable cost of doing business. In January 1898, the Bombay Plague Committee wrote that “one of the main hopes cherished by the Committee was to keep Plague within limits, which would prevent the dislocation, or even the disturbance of the general trade of the city.” For the Committee “No evil could be more fatal to trade than to allow the spread of Plague in the heart of the city, where its entire business activity centres.” Within this list of objectives, there is not a single mention of the lives of the colonised population.
Measures to control the dissemination of the plague from the port to the rest of India were only brought in after other European nations threatened to restrict Indian trade. It was only when France threatened a total ban on Indian trade and passengers and its ports that Britain conceded to the necessity to act.22 Faced with this potential catastrophe, Britain moved to placate the European nations, quickly enacting a domestic quarantine on Bombay sea traffic, and then passing the Epidemic Diseases Act in early 1897.23
The action the British did take against the plague was shaped by the racial logic through which they perceived the pandemic. For the British, the course of the plague was decided by three inherent problems in the Indian population – an innate propensity to filth, flight and riot. For these problems, the British produced three explanations – of sanitary disorder, mobile disorder and antagonistic disorder. The British response was largely shaped by an attempt to counter each of these manifestations of disorder. To counter the problem of filth, the British attacked the sanitary disorder of the city at its supposed source; the “filthy homes” of the urban poor. From February to April 1897, up to 5,000 workmen limewashed 13,891 dwellings, and destroyed ‘by fire or otherwise’ 416 more. Meanwhile, colonial officials stationed flushing engines in the street outside, to hose water and acid over the face of “infected” houses, “as if they were on fire.” This policy of disinfection to destruction reflected a belief in the almost innate filthiness of these houses, such was their contamination by their racialised inhabitants.
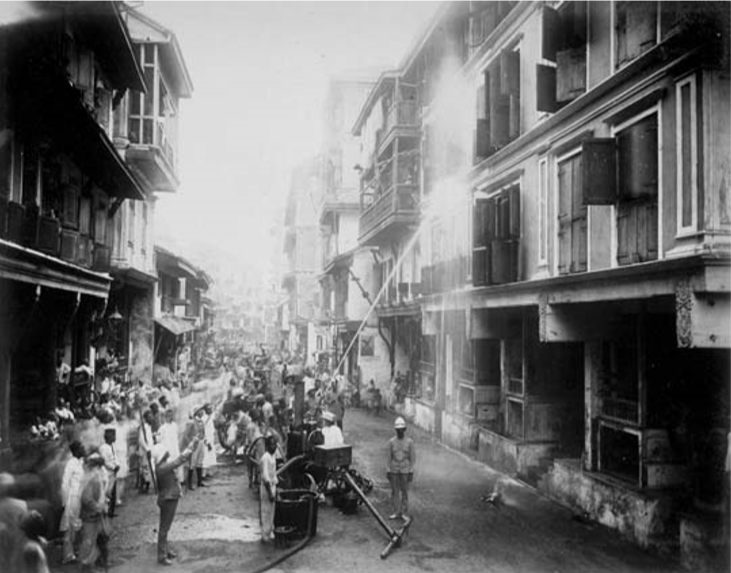
British officals direct workers operating a flushing engine, during attempts to disinfect houses in Bombay, India.
To counter the problem of flight, the British imposed a draconian regime of restriction, examination and detention. Of the 162,006 people examined on outward-bound vessels in April and May 1897, 86,938 were crew members – almost all of them Indian. This deeply racialised practice reflected an almost exclusive identification of Indians as carriers of the plague – while Indian sailors were intensively examined, European passengers were largely allowed to travel unmolested. Many of those Indians were then arbitrarily detained in huge camps by the port. A similarly racial logic guided the British attempt to counter the problem of riots. When stones were thrown at a British search party in March 1898, British policemen immediately fired two volleys into the crowd, killing nine people. As rioting spread, the British turned to the military, rapidly flooding the city with infantry, cavalry and artillery. Mass arrests and executions were used to suppress the dissent; for the British, the disorder inherent to the racialised population necessitated the violent assertion of colonial order. This then was the active part of the British response to the plague; demolitions, detentions and executions – a response defined by its constant recourse to coercion.
Denial, delay, death
Over a century later, the British response to the present pandemic has been defined, once again, by the violence of both action and inaction. Just as the British authorities in India first denied the seriousness of the plague, then delayed their response, so has the British government with coronavirus. As more cases began to emerge in Britain in February, the Health Secretary informed the press that the risk to the public “remains moderate,” while the Prime Minister assured reporters that “people have every reason to be confident and calm about all that kind of thing.” These assurances came despite dire warnings from epidemiologists and public health specialists. On March 3nd the Government was presented with a bleak warning by two modelling teams. According to their models, the current strategy of mitigation would result in around 250,000 deaths. The Government, however, did not act. In fact, they delayed taking serious action for an extraordinary twenty days. This delay would prove disastrous. On March 3rd, when the Government were first warned of the consequences of inaction, there were just 14,000 infections in the UK. By March 23rd, when the Government finally initiated a lockdown, there were 1.5 million.
The motive for these denials and delays was again the same – a fear that the economy would be negatively affected. On February 3rd, Johnson had made his opinion on the matter extremely clear;
We are starting to hear some bizarre autarkic rhetoric, when barriers are going up, and when there is a risk that new diseases such as coronavirus will trigger a panic and a desire for market segregation that go beyond what is medically rational to the point of doing real and unnecessary economic damage, then at that moment humanity needs some government somewhere that is willing at least to make the case powerfully for freedom of exchange, some country ready to take off its Clark Kent spectacles and leap into the phone booth and emerge with its cloak flowing as the supercharged champion, of the right of the populations of the earth to buy and sell freely among each other.
For Johnson, the greatest threat posed by the coronavirus was not to life, but to commerce, to the very principle of “freedom of exchange.” The active preservation of the economy involved a degree of necessary inaction; a commitment to not put up “barriers” that might interfere with the free movement of goods and people. The right of people to buy and sell was, for Johnson, more important than the health risk posed by the pandemic.
As in India, this risk was racially distributed. The same report that found that Covid-19 deaths were twice as high for racialised people as it was for whites also offered a striking and simple explanation: Britain’s racial division of labour. The report notes that a ‘third of all working-age Black Africans are employed in key worker roles, 50% more than the share of the White British population,’ while also noting that, “Pakistani, Indian and Black African men are respectively 90%, 150% and 310% more likely to work in healthcare than white British men.” The destructive effects of deep structural racism are also discussed by the report, noting the particular prevalence of underlying health conditions amongst those with a Bangladeshi, Pakistani or Black Carribean background.
The inaction which sacrifices their lives so that the white majority might continue to ‘buy and sell,’ is also, unmistakably, colonial. At the same time, when action has been taken, they too have been colonial in their form and content. Overall Black, Asian and minority ethnic people in England are 54% more likely to be fined under coronavirus rules than whites.
The particular drive of anti-Blackness is apparent in the differentiated application of the lockdown laws. In Manchester, a young black man, Gershom Leach, was issued with a fixed penalty notice and threatened with pepper spray by police officers. He was delivering food to vulnerable family members. The supposed disorder innate in the everyday activities of black people, is, for the authorities, something that must be contained with unlimited force. Meanwhile immigration officers have been given the power to detain and test people for coronavirus, ensuring the border will, once again, be differentiated in its operation, targeting racialised people while allowing whites to pass untroubled. Where there is action, it is, once again, defined by coercion.
Amidst the racial violence that defines both action and inaction, Britain chooses to remember a long-dead white hero. Nightingale’s heroism is dependent on a studied negligence, a failure to remember the work which really defined her – the pursuit of an endless coloniality, of an Empire that could last forever. This negligence ensures the continuation of the operations that defined British colonialism – the pursuit of colonial order, the brutal suppression of racialised disorder, the constant recourse to the coercive and the carceral. It is impossible to remember Nightingale as a hero without forgetting the regime she sought to protect, without forgetting the lives she was willing to sacrifice to ensure its persistence. It also impossible to commemorate Nightingale without neglecting those who die today to preserve Britain’s state of normality; the racialised nurses and doctors, drivers and pickers, upon whose labour this nation’s economy depends.
There was something inescapably colonial in the construction of the Nightingale; British soldiers building a vast hospital in a matter of days, the martial and the medical combining seamlessly, like a vision of the civilising mission. There was also something deeply colonial about its location, about building it in Newham, the borough in which 73% of the population is Black, Asian or Minority Ethnic, in which 48% of residents live in poverty, and in which the authorities have recorded the highest Covid-19 mortality rate in the country. What was most colonial about the Nightingale, however, was not its construction or location, but its operation. Despite being situated in the worst affected area in Britain, the Nightingale closed after treating just 54 patients. While impoverished, racialised people continue to die around it, the Nightingale already lies empty, with the astonishing record of having turned away more patients than it treated. Speaking on condition of anonymity, one member of staff told the Guardian that the Nightingale was never anything more than “a PR exercise, a bit of wartime propaganda.”
What wartime is this propaganda part of? What campaign is the government really fighting? The Nightingale certainly wasn’t part of any war on coronavirus; it played next to no part in preventing infection or treating the sick. Instead, this vast hospital was part of Britain’s long war on colonial memory, its counter-insurgency against both the history of the peoples it colonised in the past, and the lives of their present day descendants. The destruction of colonial history perpetuates the contemporary onslaught against racialised people; the plagues and famines of India become natural disasters, just like the tragedy in Newham. The Nightingale is a symbol of violent negligence – of the colonised people who died in India, of the racialised people left to die outside its doors. Amidst the crisis of coronavirus, this counter-insurgency rolls on unchecked. This is the message of the Nightingale – that Britain forgets the violence of yesterday so as to continue its violence today.
-
Mike Davis. 2001. Late Victorian Holocausts: El Niño Famines and the making of the Third World. London: Verso. p. 32 ↩
-
Davis. Late Victorian Holocausts. p. 36 ↩
-
Davis. Late Victorian Holocausts. p. 37 ↩
-
Jon E. Wilson. 2016. India Conquered: Britain’s Raj and the Chaos of Empire. London: Simon and Schuster. p. 243 ↩
-
Florence Nightingale. [1857]. 2006. Florence Nightingale on Health in India: Collected Works of Florence Nightingale Volume 9. Edited by Gérard Vallée. Waterloo: Wilfrid Laurier University Press. p. 49 ↩
-
Nightingale [1857], Florence Nightingale on Health in India, p. 27 ↩
-
David Arnold. 1996. Warm Climates and Western Medicine: The Emergence of Tropical Medicine 1500-1900. Leiden: Brill. p. 13 ↩
-
Nightingale. [1857]. Florence Nightingale on Health in India. p. 46 ↩
-
Nightingale. [1857]. Florence Nightingale on Health in India. p. 42 ↩
-
Nightingale. [1857]. Florence Nightingale on Health in India, p. 42 ↩
-
Nightingale. [1857]. Florence Nightingale on Health in India. p. 47 ↩
-
David Arnold. 1993. Colonizing the Body: State Medicine and Epidemic Disease in Nineteenth-century India. Berkley: University of California Press. p. 98 ↩
-
Arnold, Colonizing the Body, p. 42 ↩
-
Nightingale. [1863]. Florence Nightingale on Health in India. p. 148 ↩
-
Nightingale. [1870]. Florence Nightingale on Health in India. p. 914 ↩
-
Nightingale. [1870]. Florence Nightingale on Health in India. p. 917 ↩
-
Arnold. Colonizing the Body. p. 98 ↩
-
Arnold. Colonizing the Body. p. 203 ↩
-
Arnold. Colonizing the Body. p. 207 ↩
-
Arnold. Colonizing the Body. p. 207 ↩
-
Myron Echenberg. 2007. Plague Ports: The Global Impact of Bubonic Plague. New York: New York University Press. p. 55 ↩
-
Echenberg. Plague Ports. p. 56 ↩